

Neuro ICU > Intracranial Pressure
Intracranial Pressure (ICP)
What is ICP?
ICP is the pressure exerted on the brain by extra tissue (i.e., edema, tumor) or fluid (i.e., CSF or blood) inside the cranium. The increase in pressure (ICP) can cause brain herniation.
Why is ICP Monitored?
ICP monitoring allows the team to calculate and maintain CPP, predict outcomes, and detect worsening pathology. It is measured via an invasive probe inserted into the brain — pay attention to the parameters ordered and the readings throughout your session.
| Decision | ICP Range | Clinical Action |
|---|---|---|
| GO | 5–15 mmHg | Normal ICP. Proceed with activity as appropriate. |
| MODIFY | 16–19 mmHg | Light, in-bed activity only. Discuss with RN and/or team. Monitor closely for trends. Pressures >18 mmHg may require EVD or VP shunt intervention. |
| DEFER | ≥20 mmHg | Do not initiate activity. Notify RN. See critical thresholds below. |
Critical ICP Thresholds
ICP >25 mmHg sustained (>5 minutes): Medical emergency. Requires immediate intervention. Brief spikes above 25 may occur with stimulation or position change and do not automatically preclude therapy — trending matters.
ICP >30 mmHg: Life-threatening. Indicates poor prognosis. Do not initiate or continue therapy. Escalate to team.
Symptoms of Increasing ICP
Symptoms can include: changes in consciousness, confusion, elevated BP and slowing HR, and cranial nerve III involvement
Cushing’s Triad: a set of signs indicative of increased ICP. 1) Bradycardia, 2) irregular respirations, and 3) widened pulse pressure. Cushing's Triad is a late and ominous sign — its presence indicates the brain is already herniating and requires immediate intervention.
Causes of Increased ICP
Causes of increased ICP can include: increased BP, agitation, nausea/vomiting, increased physical exertion, supine position with HOB flat, compression of the abdomen, or the Valsalva maneuver.
Management of Elevated ICPs
External Ventricular Drain (EVD) (see lines/leads/drain section for more info on EVDs)
Hyperosmolarity therapy: hypertonic saline (3%, 23%) and Mannitol injections (20%, 25%) (see medication section for more physiological info)
Sedation
Surgical intervention: hemicraniectomy or surgical evacuation of hematoma (craniotomy)
Implications for Therapy
Mobility does not necessarily increase ICP; theoretically, sitting up should reduce ICP — however:
If the patient is not tolerating weaning of sedation due to elevated ICP (either sustained or spikes), then they may not be able to wean sedation to perform mobility/participate in therapy
Stimulation in any manner can result in elevated hemodynamics, pain, and arousal, which could elevate ICPs
Excessive neck flexion in sitting could impede normal CSF drainage & increase ICP
A change in position will cause the ICP reading to be inaccurate if the drain is not re-leveled
Coughing with a change in position, especially if the patient has an ET tube, can briefly increase ICP (increased ICP with coughing is a normal physiologic response)
If the ICP is increasing, the RN can open the EVD with the patient in a sitting position
Be sure that the patient is relatively stationary and stable in sitting if EVD is open
Video Overview
Types of ICP Monitors
(Teach Me Surgery, 2021)
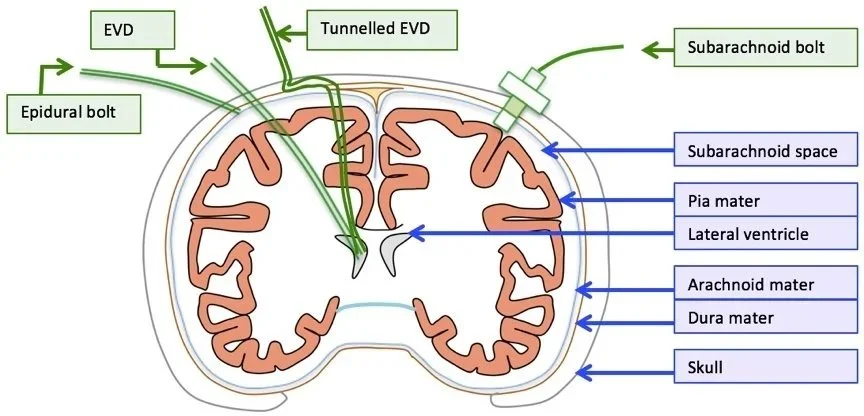
Schematic representing the anatomical insertion site for ICP monitoring
© By TeachMeSurgery, 2020
ICP Data Only (‘bolts’)
Subarachnoid Bolt/Screw: A hole is drilled in the skull, and a hollow screw is inserted abutting the dura. CSF can fill the hollow screw, allowing the pressures to equalize.
Positives: infection and hemorrhage risks are low.
Negatives: the possibility of errors from ICP underestimation, misplacement of the screw, and occlusion by debris.
Subdural/Epidural Bolt: A hole is drilled in the skull, and a sensor is inserted between the skull and dural tissue. Has decreased infection rate, but limitations include: lack of therapeutic uses, more pronounced signal attenuation, which often underestimates ICP.
**Typically, patients who have bolts in place are not stable enough to participate in therapy, but this needs to be evaluated on a case-by-case basis and could warrant further discussion with the medical team
ICP data plus CSF drainage
EVD: the gold standard for elevated ICP.
Benefits: used for therapeutic aspiration of CSF, rarely occludes, and is inexpensive.
Limitations: infection and potential for damage to the underlying brain parenchyma.
References
Clark, K. (2017). Intensive Care Unit. In H. Smith-Gabai & S. E. Holm (Eds.), Occupational Therapy in Acute Care (2nd ed., pp. 115–135). AOTA Press. https://library.aota.org/OT_in_Acute_Care_2e/134?highlightText=intensive%20care%20unit
Esbrook, C., Laxton, L., & Morrow, M. (2024). Critical care and early rehabilitation. In H. Smith-Gabai & S. E. Holm (Eds.), Occupational Therapy in Acute Care (3rd ed., pp. 115–137). AOTA Press.
Hamby, J. (2017). The Nervous System. In H. Smith-Gabai & S. E. Holm (Eds.), Occupational Therapy in Acute Care (2nd ed.). AOTA Press.
Pinto, V. L., Tadi, P., & Adeyinka, A. (2021). Increased Intracranial Pressure. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK482119/
Teach Me Surgery. (2020, October 29). Intracranial pressure monitoring. TeachMeSurgery. https://teachmesurgery.com/neurosurgery/flow-and-pressure/icp-monitoring/