

ICU Topics > Considerations & Contraindications
Considerations & Contraindications
Therapy appropriateness in the ICU is a daily clinical decision driven by the patient's full picture — not a single threshold. This page covers the condition-specific nuance behind that decision: devices, medical complications, sedation status, and other factors that shape whether a patient is ready for therapy on a given day.
For the GO/MODIFY/YIELD/DEFER/STOP decision tiers, see Activity Decision Framework.
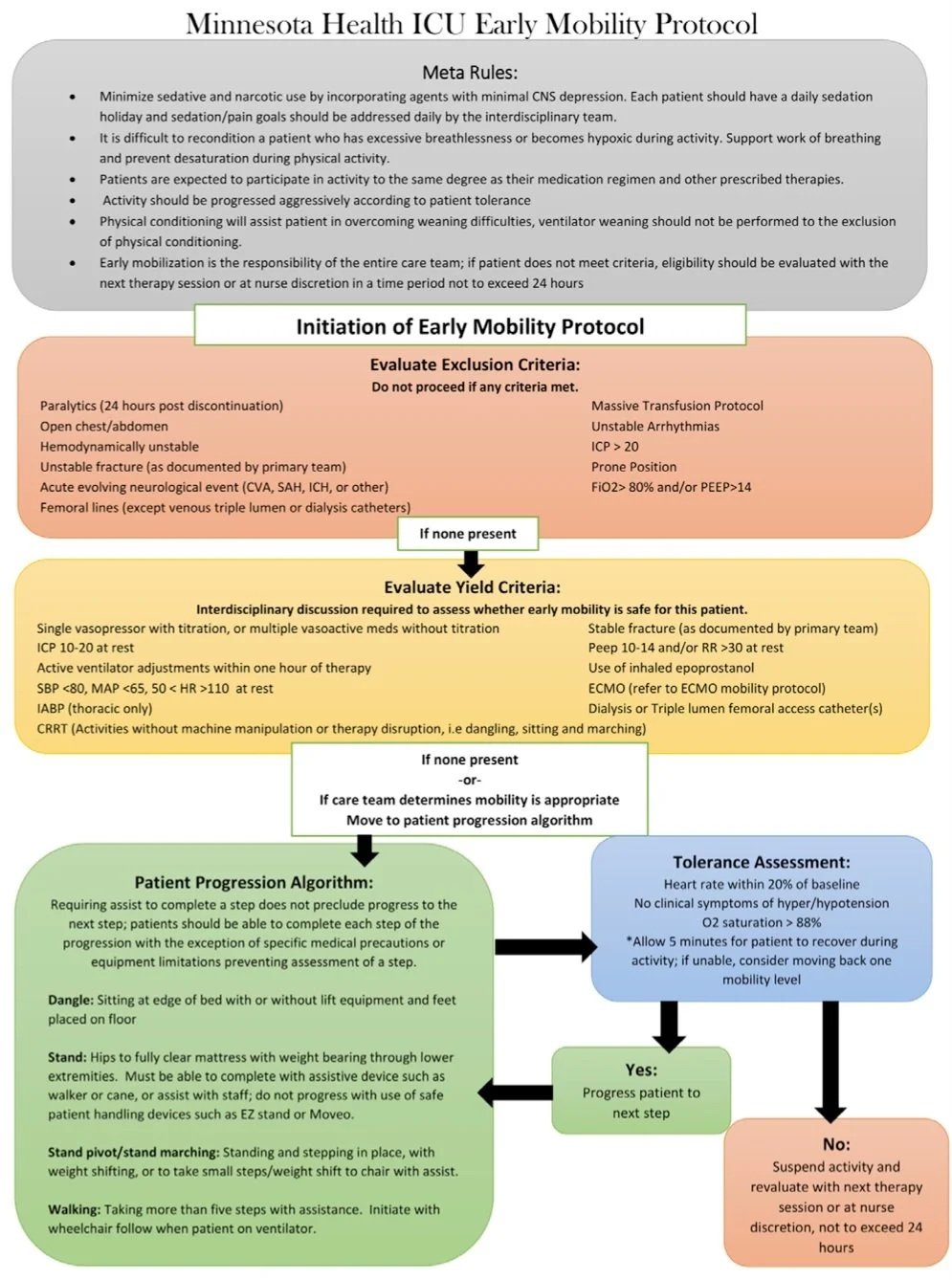
An inclusion/exclusion algorithm to support clinical reasoning is available below (Linke et al., 2020).
Algorithm to guide clinical reasoning (Linke et al., 2020)
Clinical Reasoning Principle
- These criteria are a starting point, not a finish line. Always assess in context.
- Trends matter more than single numbers. A MAP of 66 dropping for 2 hours is not the same as a MAP of 66 that has been stable all day.
- A single red criterion overrides all green ones.
- When in doubt, yield. Consult the team, document your reasoning, and reassess.
- The goal is to maximize activity safely — not to find reasons to exclude patients.
Hodgson et al., 2014
Image used with permission from the author
Other General Considerations
-
*Not yet treated with anticoagulants
A DVT occurs when a blood clot forms in a deep vein, usually the lower leg, thigh, pelvis, or arm. New, untreated DVT is a reason to defer mobility until medical management is clarified.
Signs & symptoms: Pain and swelling distal to the thrombus, localized redness and warmth, low-grade fever, dull ache or tightness in the region of the DVT.
Diagnostic testing: Upper or lower extremity non-invasive study (UENIS/LENIS)
Clarify plan for medical management before treating. The patient may be appropriate for therapy if anticoagulation has been started (e.g., Heparin, Lovenox, Fragmin, Coumadin) or if an inferior vena cava (IVC) filter has been placed.
(Centers for Disease Control, 2020; Engel et al., 2013)
-
*Not yet treated with anticoagulants
A PE occurs when part of a clot breaks off and travels to the lungs, causing a blockage. It is a serious complication of DVT. New, untreated PE is a reason to defer until anticoagulation is in place.
Signs & Symptoms: Tachycardia, possible chest pain, rapid onset of tachypnea, anxiety, lightheadedness, dysrhythmia, hypotension, and decreased oxygen saturation.
Clarify the plan for medical management before treating. The patient may be appropriate for therapy if anticoagulation has been started (e.g., Heparin, Lovenox, Fragmin, Coumadin) or if an IVC filter has been placed.
(Centers for Disease Control, 2020)
-
The following devices warrant caution or team discussion before mobilizing:
Femoral intra-aortic balloon pump (IABP)
ECMO
Ventricular assist device
Pulmonary artery catheter or other cardiac monitoring device
Venous or arterial femoral catheters
Femoral sheaths
Continuous renal replacement therapy (CRRT)
(Rawal & Bakhru, 2024)
-
Earlier rehabilitation is generally better. The following factors can help guide your assessment of whether a patient is ready for OT evaluation.
Indicators of readiness:
ICP is controlled (if a bolt is in place, verify with team — some neurosurgeons allow mobilization with close monitoring)
Blood pressure is stable at rest (some fluctuation with activity is expected)
Sedation has been weaned, lightened, or turned off for evaluation
Medical confounders are being actively treated
Factors suggesting the patient is not yet ready:
Persistent ICP >25 mmHg with active hyperosmolarity therapy
Medically paralyzed (neuromuscular blockade)
Team or nursing concerns about medical stability
Specific orders prohibiting sedation lightening
Scheduled goals-of-care or comfort-measures discussion with anticipated change in code status
(Hodgson et al., 2014; Linke et al., 2020)
-
Patients on mechanical ventilation can participate in therapy, but require careful monitoring and a lower threshold to modify or stop activity.
During weaning: Be cautious when progressing activity during the ventilator weaning period — the increased respiratory demand of exercise may reduce tolerance. Monitor closely for signs of respiratory distress: autonomic changes, paradoxical breathing, tachypnea, agitation, diaphoresis, cyanosis, or arrhythmias.
Prolonged MV risk: Patients requiring prolonged mechanical ventilation are at elevated risk for respiratory muscle atrophy, skin breakdown, contractures, and deconditioning — making early activity more important, not less.
Note on PEEP and FiO₂: Higher PEEP (>10–14 cmH₂O) and FiO₂ (>60–80%) shift the decision toward MODIFY or YIELD. Always note current vent settings in your chart review before entering the room.
(Hodgson et al., 2014; Linke et al., 2020)
-
Post-operative patients recovering from general anesthesia require additional monitoring. The effects of anesthesia can persist and complicate therapy participation.
General physiological effects:
Neurological: Decreased cortical and autonomic function
Cardiovascular: Potential for arrhythmias, decreased BP, decreased myocardial contractility, reduced peripheral vascular resistance
Respiratory: Decreased arterial oxygenation, decreased surfactant, diminished airway reflexes
Common post-operative complications to monitor:
Neurological: Delayed arousal, agitation, altered consciousness, cerebral edema, seizure, stroke, peripheral weakness
Cardiovascular: Hypotension, hypertension, dysrhythmia, MI, DVT, PE
Respiratory: Airway obstruction, hypoxemia, hypercapnia, pulmonary edema
General: Acute renal failure, urinary retention, abdominal distention, hypothermia, sepsis, hyperglycemia, fluid imbalance, acid-base disorders, post-operative pain
(Clark, 2017; Holm, 2017)
-
Many ICU patients experience barriers to effective communication due to intubation, pharmacologic sedation, neurological impairment, or musculoskeletal limitations. Identifying these barriers before the session allows you to plan your approach.
Factors that influence communication ability:
Level of arousal and cognitive status (RASS, CAM-ICU)
Physical limitations (UE weakness, positioning)
Visual or hearing impairments (glasses, hearing aids present?)
Speech or language impairments
Literacy and ability to recognize letters, numbers, or familiar images
Language barriers — interpreter services needed?
Alternative and augmentative communication (AAC) strategies:
Yes/no head nodding or hand gestures
Communication board (letters, words, images)
Eye gaze or blink systems for non-verbal patients
Passy-Muir Valve (PMV) for tracheostomized patients — allows voicing through a one-way valve (speech-language pathology consult often coordinates this)
(Clark, 2017)
-
Before entering the room, check in with the bedside nurse and review the most recent RASS score. Use these questions to frame your decision:
Can I see my patient? Are they:
"Sedated but arousable" — possibly appropriate; warrants discussion with RN
"Sedated but follows commands" — likely appropriate
"Deep sedation" — likely not appropriate
"Minimally sedated" — possibly appropriate; warrants discussion with RN
"Agitated, frequently pulling at lines" — likely not appropriate
"Sedation increased to improve synchrony with the vent" — not appropriate
Remember: appropriateness fluctuates. A patient who was too agitated yesterday may be appropriate today — and vice versa. Check the RASS every session.
(Hodgson et al., 2014; Linke et al., 2020)
References
Brummel, N. E., Jackson, J. C., Girard, T. D., Pandharipande, P. P., Schiro, E., Work, B., Pun, B. T., Boehm, L., Gill, T. M., & Ely, E. W. (2012). A combined early cognitive and physical rehabilitation program for people who are critically ill: The activity and cognitive therapy in the intensive care unit (ACT-ICU) trial. Physical Therapy, 92(12), 1580–1592. https://doi.org/10.2522/ptj.20110414
Centers for Disease Control. (2020, February 7). What is venous thromboembolism? Centers for Disease Control and Prevention. https://www.cdc.gov/ncbddd/dvt/facts.html
Clark, K. (2017). Intensive Care Unit. In H. Smith-Gabai & S. E. Holm (Eds.), Occupational Therapy in Acute Care (2nd ed., pp. 115–135). AOTA Press. https://library.aota.org/OT_in_Acute_Care_2e/134?highlightText=intensive%20care%20unit
Engel, H. J., Needham, D. M., Morris, P. E., & Gropper, M. A. (2013). ICU early mobilization: From recommendation to implementation at three medical centers. Critical Care Medicine, 41, S69–S80. https://doi.org/10.1097/CCM.0b013e3182a240d5
Giacino, J. T., Whyte, J., Nakase-Richardson, R., Katz, D. I., Arciniegas, D. B., Blum, S., Day, K., Greenwald, B. D., Hammond, F. M., Pape, T. B., Rosenbaum, A., Seel, R. T., Weintraub, A., Yablon, S., Zafonte, R. D., & Zasler, N. (2020). Minimum competency recommendations for programs that provide rehabilitation services for persons with disorders of consciousness: A position statement of the American congress of rehabilitation medicine and the national institute on disability, independent living and rehabilitation research traumatic brain injury model systems. Archives of Physical Medicine and Rehabilitation, 101(6), 1072–1089. https://doi.org/10.1016/j.apmr.2020.01.013
Hamby, J. (2017). The Nervous System. In H. Smith-Gabai & S. E. Holm (Eds.), Occupational Therapy in Acute Care (2nd ed.). AOTA Press. https://library.aota.org/OT_in_Acute_Care_2e/134?highlightText=intensive%20care%20unit
Holm, S. (2017). Early Mobility and Rehabilitation. In H. Smith-Gabai & S. E. Holm (Eds.), Occupational Therapy in Acute Care (2nd ed., pp. 663–672). AOTA Press. https://library.aota.org/OT_in_Acute_Care_2e/134?highlightText=intensive%20care%20unit
Linke, C. A., Chapman, L. B., Berger, L. J., Kelly, T. L., Korpela, C. A., & Petty, M. G. (2020). Early mobilization in the ICU: A collaborative, integrated approach. Critical Care Explorations, 2(4), e0090. https://doi.org/10.1097/CCE.0000000000000090
Mendez-Tellez, P. A., & Needham, D. M. (2012). Early physical rehabilitation in the ICU and ventilator liberation. Respiratory Care, 57(10), 1663–1669. https://doi.org/10.4187/respcare.01931
Oldenburg, H. Y., & Hamby, J. R. (2024). The novice in acute care. In H. Smith-Gabai & S. E. Holm (Eds.), Occupational Therapy in Acute Care (3rd ed., pp. 927–961). AOTA Press.
Rawal, H., & Bakhru, R. N. (2024). Early mobilization in the ICU. CHEST Critical Care, 2(1), 100038. https://doi.org/10.1016/j.chstcc.2023.100038